Growing up, I probably ate close to a thousand McDonald’s cheeseburgers. They were my favorite food, bar none. Sure, the Happy Meal toy didn’t hurt, but something about the pale orange American cheese (which technically can’t be considered real cheese), thin, processed patty, and pillowy, artificial bun just spoke to the heart and palate of young Ethan.
Every time my dad took me, he’d get something to eat too. And like clockwork, in the drive-thru, my dad would think about getting a burger, say out loud “no that’s got too much cholesterol,” and order a Filet-O-Fish.
Never mind that the Filet-O-Fish has deep fried fish, cheese and creamy, cholesterol-rich tartar sauce, causing it to have only 10 mg less cholesterol than the burger. Just the specter of high cholesterol from the burger was enough to dissuade my dad.
And that specter is unfortunately well-earned. A tremendous body of evidence from over the past several decades has identified a powerful association between elevated cholesterol levels and cardiovascular disease. And don’t forget, cardiovascular disease is the leading cause of mortality globally, not just here in the U.S. As such, cholesterol levels are one of the most important risk factors that physicians and patients must manage in order to preserve their cardiovascular health and avoid morbidity (disease) and mortality (death).
The mechanisms that underlie this association are complex. First off, it’s important to understand that in the body, cholesterol isn’t just floating around and chilling solo. What gets measured on a blood test are the packages holding cholesterol, called lipoproteins. There are many different kinds of lipoproteins, but the one that keeps cardiologists up at night is LDL, or low-density lipoprotein.
LDL is made in the liver, and its job is to deliver cholesterol to peripheral tissues. Their level is regulated by the liver as well, and if the liver senses that there is too much cholesterol in the body, the liver can create more LDL receptors that snatch LDL from the blood and prevent it from depositing LDL in the body. LDL particles are considered “bad” because they are extremely rich in cholesterol and deposit said cholesterol all over the body, most concerningly in blood vessel walls.
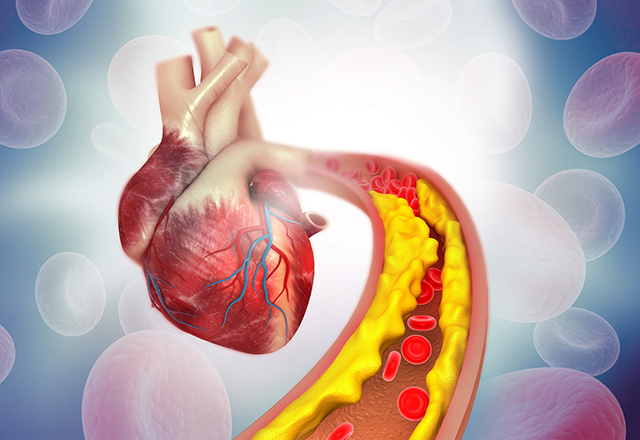
This cholesterol deposition in the walls of blood vessels is what underlies the connection between elevated LDL and cardiovascular disease. As cholesterol accumulates in the walls of blood vessels, like gunk accumulating in a pipe, it slowly occludes blood vessels. Additionally, this cholesterol isn’t inert. Research has shown that as LDL travels to and deposits cholesterol in blood vessel walls, it induces inflammation and oxidative stress on blood vessel tissue.
These cholesterol deposits, called plaques, over time form a core of lipids and a hard outer shell of collagen. The worst-case scenario, which can induce a heart attack, is when this plaque ruptures. If the collagen shell is broken, the lipid core becomes exposed, and this leads to the formation of a clot, which can fully obstruct a blood vessel and cause significant damage.
That’s why internists and cardiologists focus so much on controlling LDL, because elevated LDL is like a ticking time bomb. With elevated LDL, more and more cholesterol plaques form. These plaques through their size alone can partially occlude vessels, but also present the possibility of rupturing and causing a catastrophic complete occlusion. If this complete occlusion happens in the small blood vessels that supply the heart muscle, the heart muscle can die. That is the mechanism of a heart attack.
Internists and cardiologists have an armament of medications to treat elevated cholesterol — 35% of Americans report taking a statin (drugs like atorvastatin or rosuvastatin), the first-line treatment for high cholesterol. But unfortunately, for a large proportion of Americans, these haven’t been enough. Further, as evidenced by my dad, cholesterol isn’t some secret, and the importance of controlling cholesterol is widely popularized in the general public and by medical professionals. Despite this, high cholesterol persists as a serious public health problem. Estimates vary, but what’s clear is that millions of Americans still have high cholesterol. A paper in JAMA Cardiology cites that a little over 8% of Americans have high LDL, over 160, while the AHA estimates that 25.5% of U.S. adults have high LDL, defined as LDL over 130. While our current tools work, it’s clear that we need more.
Enter PCSK-9 inhibitors, the new kid on the block in the world of cholesterol control. PCSK-9 is a protein that plays an important role in regulating the LDL receptor, which if you recall, is important in snatching up excess LDL from the blood. Experiments with PCSK-9 show that PCSK-9 works by binding to the LDL receptor and dragging it to lysosomes, where they are degraded. As such, PCSK-9 works like an anti-LDL receptor. As PCSK-9 activity increases, LDL receptors decline. With fewer LDL receptors, less LDL is snatched from the blood, and more LDL is allowed to circulate in the blood and deposit cholesterol in tissues and blood vessels.
It’s a bit convoluted, but in short, PCSK-9 activity is correlated with higher LDL cholesterol. Therefore, by inhibiting PCSK-9 with a PCSK-9 inhibitor, which in turn increases the amount of active LDL receptors that can snatch LDL cholesterol from the blood, we can decrease the amount of LDL in the blood.
The beauty of these medications is that they can work hand-in-hand with our existing armament of cholesterol-lowering medicines. When I rotated on general cardiology here at Hopkins, I saw patients on the highest doses of statin medicines and another cholesterol medicine called ezetimibe. Many patients still had high LDL. The cardiologists prescribed PCSK-9 inhibitors, either Repatha or Praluent, and the combination of all three medicines worked to help lower cholesterol.
The impact isn’t minor either. Clinical trials have shown a decrease in LDL of 57% and 59% with the use of the two PCSK-9 inhibitors, which is similar to the impact of starting a high-intensity statin, the first-line treatment for high cholesterol. Crucially, these clinical trials for PCSK-9 inhibitors included patients already on cholesterol-lowering therapy like statins, meaning that this impact is additive, on top of the reductions already provided with existing medicines.
But LDL is just a lab value. The ultimate goal of these drugs is to prevent cardiovascular disease, and the studies support an association there. Those same clinical trials studying PCSK-9 inhibitors found that patients taking the medicines experienced 15%–21% reductions in the incidence of major cardiovascular events like heart attacks. On a population-wide scale, this translates to many heart attacks avoided and lives saved.
They also generally have a benign side effect profile, with the most common side effects being injection-site reactions like bruising, muscle-related issues like aches/pains, or flu-like illness. While I don’t mean to discount these side effects, it’s important that these drugs, as of now, haven’t shown links to side effects that persist with time or cause significant, long-term damage.
The downside of these drugs is that they are expensive injection medications. PCSK-9 inhibitors can be the greatest drugs in the world, but if people aren’t taking them, it doesn’t really matter. The list price for Repatha, for example, is $572.70 per month. Patients have to initially go to the doctor to receive and learn how to administer these shots, and have to continue receiving these injections every two to four weeks. This isn’t a trivial concern. Fear of needles is very common, which is a barrier to initiating and adhering to these medicines. Further, the aforementioned injection site reactions are both in themselves burdensome and serve as another barrier to adherence to these medicines.
These issues with adherence are not just theoretical. An analysis of patients prescribed PCSK-9 inhibitors showed that only 49.9% of patients paid for and actually received their PCSK-9 medication, compared to the high 60s to 80s for other cardiometabolic drugs. Cost certainly contributes to this, but the combination of inconvenience/fear that comes with its route of administration certainly doesn’t help.
In regard to the cost, the list price of PCSK-9 inhibitors has fallen 60%, but copays that patients have to pay are still elevated. Increasing insurance coverage and decreasing copays here will be critical. But in regard to the issues with injections, that may be changing.
In a new randomized controlled trial, a novel oral PCSK-9 inhibitor named AZD0780 (what a catchy name) was compared against placebo in 428 patients with elevated LDL and already on statin therapy. The medication was given once daily, and the highest dose tested (30 mg) was associated with a 50.7% reduction in LDL levels compared with placebo after 12 weeks. The efficacy scales with dose, with lower doses correlating with lower reductions in LDL levels. Reminder, the reduction we saw with the injection PCSK-9 inhibitors was 57%–59%, meaning that this oral drug at 30 mg daily is comparable. That’s huge.
But there was more to the study. They also checked for side effects, and the rate of adverse events was only slightly elevated (38.2% versus 32.6%) compared to placebo. You might ask, how does a placebo cause 32.6% of people to get side effects? It’s important to remember that these patients were already on statins, which themselves can cause many side effects, similar to those reported by PCSK-9 inhibitors. Adverse events reported in this study also were not severe events, and included issues like abdominal pain or headache. Patients received blood and urine tests, heart electrical scans called EKGs, and measured vitals, and only one participant noted any concern, which was an elevation in a marker of liver function. They did not exhibit symptoms of liver dysfunction, though.
However, it’s important to not get too excited. This study was a Phase 2 study, meaning that the goal was mostly to determine whether the treatment was effective. It’s not enough to say we should start deploying this drug nationwide, because we need more research on the drug’s effectiveness and — importantly — safety, on a larger scale. A Phase 3 trial, with thousands of participants is still needed, because it’s entirely possible that some rarer side effect was missed by this Phase 2 study. But it’s still promising, and further so because this isn’t the only candidate in this drug class.
In a review article on oral PCSK-9 inhibitors published in September, authors identified two other randomized controlled trials of novel oral PCSK-9 inhibitor candidates, conducted in 2023 and 2024. At their maximum doses studied, both of these other candidates (MK-0616 and NNC0385-0434) showed similar, dramatic reductions in LDL levels (60.9% and 61.8% respectively) to the AZD0780 drug we discussed previously. Neither of these drugs were reported to have increased risk of serious adverse effects either. Similarly though, these were Phase 2 studies. But the fact that three drug candidates with similar mechanisms all showed effectiveness and lacked any significant safety signals in Phase 2 trials is another promising sign that this oral drug class might actually pan out.
In closing, high cholesterol is a serious public health issue. When doctors talk about it, they’re usually referring to LDL, which deposits cholesterol all over the body, but most concerningly in blood vessels, where plaques can form and rupture to cause heart attacks. We have a lot of medications to treat high cholesterol, but it remains elevated in a large number of people, so new drugs, like PCSK-9 inhibitors, are greatly needed.
My dad still doesn’t eat cheeseburgers from McDonald’s. But say he decided to, and his cholesterol got out of control, I’d be happier knowing he had another tool in the toolbox, like an oral PCSK-9 inhibitor, to get it under control, and I’m sure countless doctors and their patients would too.
Related Content
- Reflections on Aging and Geriatrics
- Building the Bridge from Medicine 2.0 to Medicine 3.0
- The Need to Diversify Narrative Medicine
Want to read more from the Johns Hopkins School of Medicine? Subscribe to the Biomedical Odyssey blog and receive new posts directly in your inbox.