
Why Winners Keep Winning
You are on a roll. In the morning, you delivered a compelling business proposal. You were the center of attention at lunch and your colleagues… Read More »Why Winners Keep Winning
You are on a roll. In the morning, you delivered a compelling business proposal. You were the center of attention at lunch and your colleagues… Read More »Why Winners Keep Winning

Glioblastoma research is similar to superhero film plots. How, you may ask? If each superhero represents a different treatment drug, then we as researchers want… Read More »Advancing Glioblastoma Research: A Tale of Two Superheroes
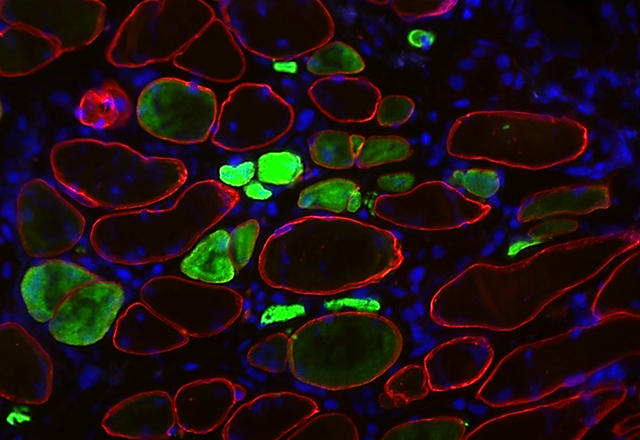
If you were diagnosed with a disease, there are two questions you would immediately want answered: 1. How can we treat it? 2. What caused… Read More »Developing a Laboratory Model for Inclusion Body Myositis

Stepping into the Anne and Mike Armstrong Medical Education Building (AMEB), you can always count on Aisha to brighten your day. Born and raised in… Read More »Hidden Talent at Hopkins

Medical school curriculum has traditionally been split into two halves: preclinical and clinical years. Preclinical years generally include the first two years of medical school,… Read More »The Beginning and End of an Era

A patient develops symptoms that cannot be explained. The doctor orders a myriad of tests to discern the cause. If cancer is suspected, the patient… Read More »A New Blood Test Tries to Detect Cancer Sooner

Biology is a vast and rapidly evolving field. The science of life ranges from studying the physical and chemical interactions of molecules to mapping a… Read More »Drowning in Data: New Challenges in Modern Biology
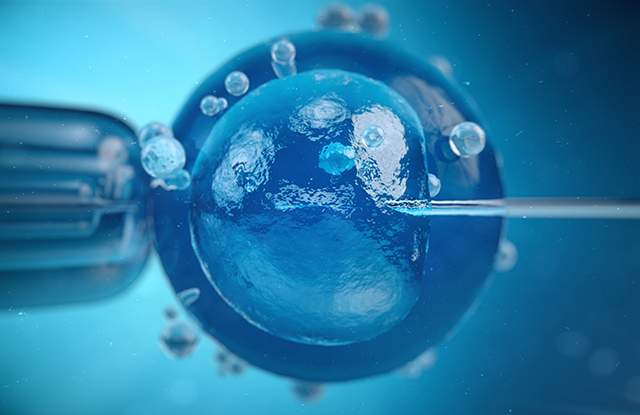
About 40 years ago (July 1978), Louise Joy Brown was born at Oldham General Hospital in England, weighing 5 pounds, 12 ounces. This birth may… Read More »Fresh or Frozen Embryos? Equal Live-Birth Rates Among Infertile Women

Do you blog? Journal? Write in your spare time? Are you interested in pursuing communications at any level in parallel with your professional training? We need you!… Read More »Do You Want to Write For Us?

Toxic stress is everywhere. As a pediatrician in Baltimore City, I acknowledge the elephant in the exam room at nearly every appointment. Abuse. Neglect. Domestic… Read More »Mental Health on the Reservation: Native American Teens and Toxic Stress